Trying to understand why physicians make the decisions they do is critically important in pharmaceutical market research. An assessment of market dynamics forms the underpinning for virtually all of marketers’ strategic and tactical decisions supporting their brand.
Yet even when the brand team has commissioned and completed market dynamics research, they often find themselves taken by surprise when a product launch doesn’t go as well as expected or a promotional strategy seems to miss the mark. Market research can fall short in any number of ways, but one critical shortcoming in market dynamics research is an incomplete appreciation of non-rational drivers of behavior. In this paper, we describe these drivers and why they’re important, and highlight some techniques for uncovering them in market research.
Rational and Non-Rational Decision Drivers: An Illustration
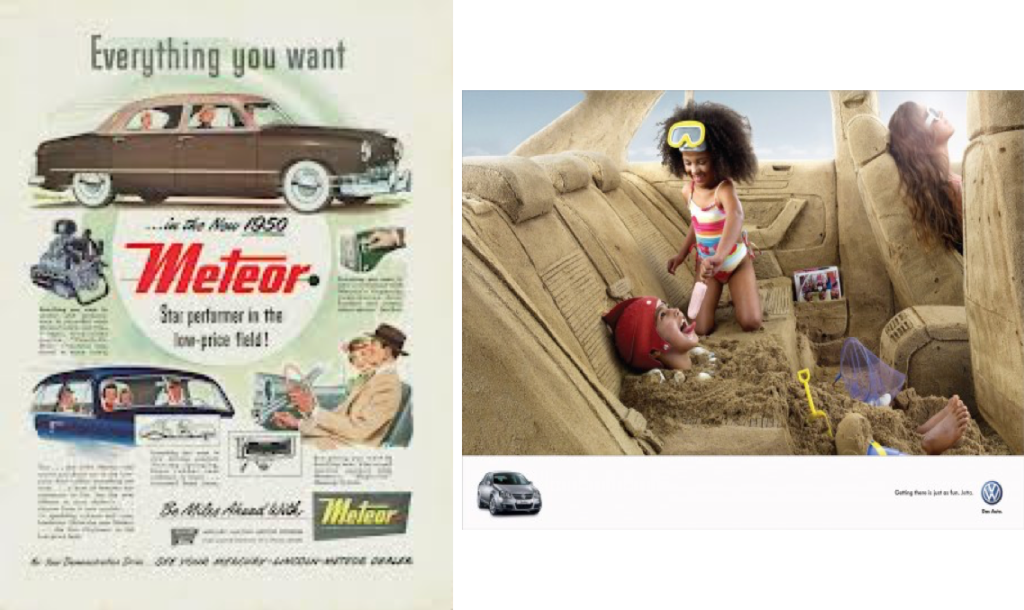
The two car ads below illustrate how marketers can appeal to the rational and the non-rational sides of our decision-making. The vintage ad on the left is highly rational, focused on facts; its goal is to sell the consumer on the rational benefits of the car. The modern ad on the right provides no facts at all – its goal is to create a feeling and give the brand a personality, drawing the consumer in via a non-rational path.
It’s almost as if the vintage and modern ads were created for totally different people, whose brains make decisions in totally different ways. And in a sense, that’s true – except that both of these brains reside in each of us. Different areas of our brains process information so differently that’s its not much of a stretch to think of them as different brains.
This model of information processing has been called the “triune brain” (setting aside for our purposes a recently identified fourth area and the corresponding “quadrune brain” label). The triune model recognizes that as humans evolved to develop more sophisticated and rational ways of processing information, these newer ways of thinking did not replace the older information processing systems. Instead, they developed alongside of the older systems.
All three ‘brains’ process information and guide behavior, but in different ways: the brain stem focuses on survival and safety, the limbic system on emotions and social connections, and the neocortex on setting goals and planning rationally. And often, when the areas are in disagreement (e.g., the neocortex puts us on a diet, but the limbic system demands dessert), the result is non-rationally driven behavior.

Doctors are people too
Most of us (including marketers) are comfortable thinking about patient/consumer choices in this way; consumer-oriented marketing efforts almost always target the non-rational brain, at least in part. But promotions to physicians rarely do. While we’d never equate physicians’ decisions about which drug to prescribe with teenagers’ decisions about which brand of shoe to buy, it’s nonetheless true that physicians have the same triune brain as the rest of us. We can see it in their own health behaviors: just like the rest of us, many physicians fail to exercise or eat enough fruits and vegetables (and consequently are overweight).

Implications for market research
If physicians’ decisions can be non-rational, then market dynamics will reflect non-rationality. We should therefore design market research to understand both rational and non-rational drivers of decision-making. This can be challenging, because physicians try to appear purely rational, and traditional market research approaches play into this bias.
We’ve found that we can learn about non-rational dynamics—sometimes with profound implications—through relatively simple exercises. One helpful approach is through an archetype analysis of customer journey interviews. Archetypes are shared cultural stories that carry a rich network of associations. They organize psychological impulses and direct them in meaningful ways; when a particular archetype is activated, its pull on behavior is strong.
A recent example illustrates how powerful archetype analysis can be. In 2013, we conducted research to help understand why a recent product launch in the cardiovascular space had not gone as well as expected. Sales for the product lagged expectations significantly; this was particularly puzzling because the team believed they had better data than any competitor.
To help us understand how physicians thought of themselves at a non-rational level, we talking to them what they find satisfying and challenging about being a physician. We also talked to them about why they decided to become a physician in the first place and what led them to chose their specialty. Finally, we talked to them about what it’s like treating the CV conditions of relevance to our client. Analysis of this information revealed that physicians fell into one of three archetypes: The Hero, The Sage, or The Caregiver.

Physicians operating under these different archetypes used the client’s product very differently. The two extremes are The Sage and The Hero; whereas The Sage responded positively to the data-heavy promotion with strong uptake, The Hero did not. Heroes rely on their own experience over clinical trial data, and they take decisive action without over-thinking. They view themselves as gifted problem-solvers and want their patients and sales reps to treat them accordingly; they get frustrated when those around them don’t treat them with the respect they think they deserve.
Armed with this understanding of The Hero archetype, these physicians’ low rates of prescribing the new product suddenly made sense. Their reliance on personal experience over clinical trials explains why they failed to respond to strong clinical trial data. Their personal frustration with non-adherent patients also had implications for brand choice. So whereas low uptake of the client’s product was puzzling from a purely rational point of view, it was completely understandable once we understood non-rational market dynamics. These insights helped us identify an appropriate set of solutions for the brand team.
Implications for the evolving cholesterol market
From a purely rational point of view, the change in AHA/ACC guidelines for treating cholesterol (from reaching specific goals to using specific doses of specific drugs to reach a desired percent-change) could a game changer. However, early indications suggest that prescribing patterns haven’t changed that much.
How can that be? We believe it is because non-rational dynamics haven’t changed, and those have been important all along. In fact, we would argue that the new AHA/ACC recommendations represent an attempt to codify (and therefore make rational) a market dynamic that is fundamentally non-rational: namely that physicians in general—and perhaps cardiologists in particular—don’t like to feel like failures. They don’t like goals they can’t achieve, and reaching an LDL of 70mg/dL often seems unachievable. So perhaps the thinking behind the change was a non-rational one: if we can’t get our patients to reach the goal, then we should change the goal to something we can attain.
This hypothesis is based on the many hundreds of qualitative interviews we’ve conducted over the past 10+ years. It’s also supported by the fact that the new AHA/ACC guidelines were not brought about by new data or evidence. Indeed, a large body of clinical trials consistently shows that lowering LDL to 70mg/dL or below significantly reduces CV events—a fact not overlooked by the National Lipid Association, which broke from the AHA/ACC in rejecting the new cholesterol guidelines.
A final clue comes from cardiologists’ reactions to the new guidelines, as reported in the media. Many express relief that they will no longer have to “chase targets.” (an odd sentiment in an age of evidence based medicine). The statement by Dr. Stone, chairman of the panel in charge of the new guidelines, is also telling: he comments that the guidelines solve the problem of patients feeling like failures for not reaching goal. One can’t help but wonder if he hasn’t shared this feeling of failure in the past, and that this personal feeling of failure wasn’t a driver of the guideline changes. Then again, that wouldn’t be rational!